Surgical Hair Loss Treatment
For many people, a hair transplant can help bring back a fuller head of hair.

What is it?
Follicular unit extraction (FUE) hair transplants are done by taking individual hair follicles out of your donor area and implanting them elsewhere in your recipient area. This will make the hair in the recipient area look thicker.
- Restored hair line
- Restored Confidence
Who’s it for?
The best candidate for a FUE hair transplant is someone with thinning hair who still has enough donor hair to use for a transplant.
- Generally over 30
- Where medication is insufficient alone

The Process
It’s a one day out-patient procedure requiring only local anesthesia. Most patients are surprised by how little discomfort, if any, they experience during and after surgery. Many patients simply relax during their hair transplant procedure.
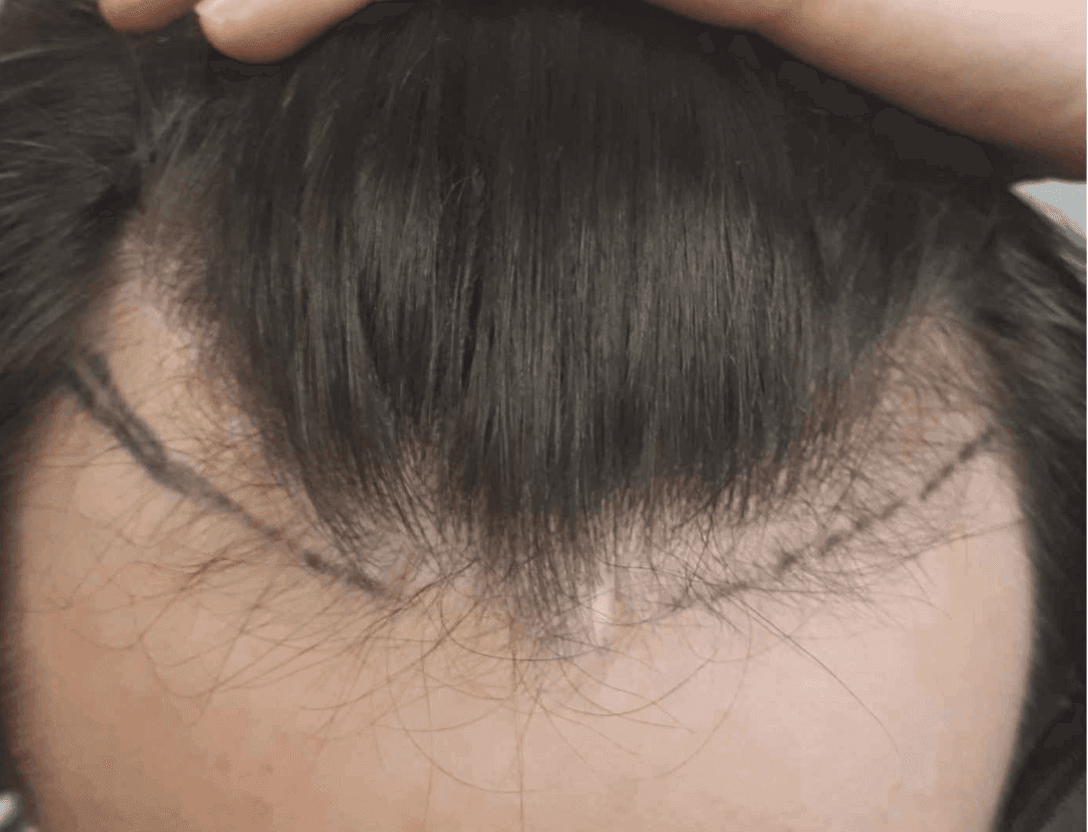
We shave the recipient and donor areas in preparation for surgery
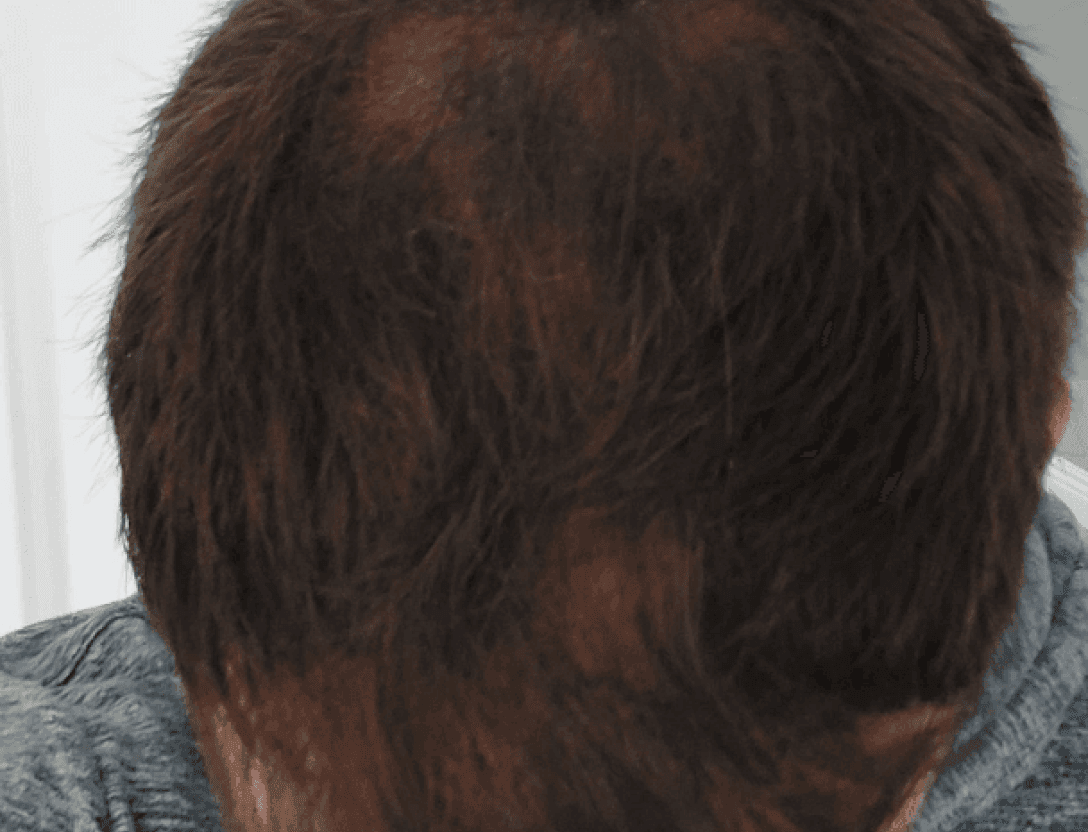
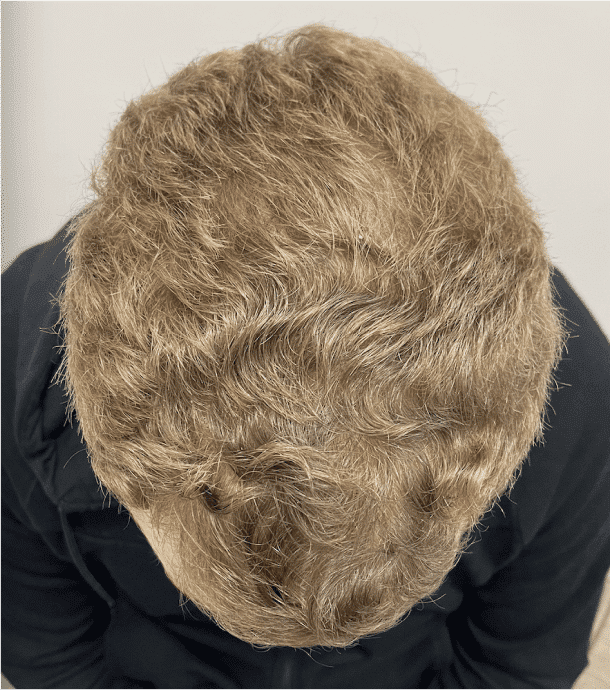
Hair restoration that change lives


Received 1,500 grafts with a total of 4,300 hairs transplanted .









































Treatment Cost
The treatment cost varies depending on the number of grafts taken for each patient's individual needs. Generally, the amount approximately ranges from €2,000 to €4,000.
Our doctor will provide you with the final treatment cost during the consultation session if surgery is the right option for you.
Common Questions Asked
Complete our free online consultation to receive advice from our doctor who will provide you with a clear treatment path tailored for you